
Page 30 - total-knee-packet
P. 30
Dr. Christian Eccles
Hip and Knee Replacement Surgery
2940 E. Banner Gateway Dr. #200, Gilbert, AZ 85234
1675 E Melrose St, #101, Gilbert, AZ 85297
Phone: 480.964.2908 | Fax: 480.388.3519
Medical Assistant (Reese) extension: 3186
Surgery Scheduler (Debbie) extension: 4141
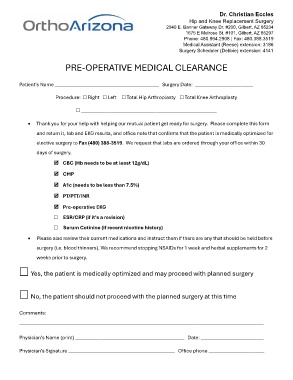
PRE-OPERATIVE MEDICAL CLEARANCE
Patient’s Name ___________________________________________ Surgery Date: ________________________
Procedure: ☐ Right ☐ Left ☐ Total Hip Arthroplasty ☐ Total Knee Arthroplasty
☐ ________________________________________________________
• Thank you for your help with helping our mutual patient get ready for surgery. Please complete this form
and return it, lab and EKG results, and office note that confirms that the patient is medically optimized for
elective surgery to Fax (480) 388-3519. We request that labs are ordered through your office within 30
days of surgery.
CBC (Hb needs to be at least 12g/dL)
CMP
A1c (needs to be less than 7.5%)
PT/PTT/INR
Pre-operative EKG
☐ ESR/CRP (if it’s a revision)
☐ Serum Cotinine (if recent nicotine history)
• Please also review their current medications and instruct them if there are any that should be held before
surgery (i.e. blood thinners). We recommend stopping NSAIDs for 1 week and herbal supplements for 2
weeks prior to surgery.
☐ Yes, the patient is medically optimized and may proceed with planned surgery
☐ No, the patient should not proceed with the planned surgery at this time
Comments:
_____________________________________________________________________________________________________
Physician’s Name (print) _____________________________________________ Date: __________________________
Physician’s Signature ____________________________________________ Office phone _______________________